Recent Amulet paper:
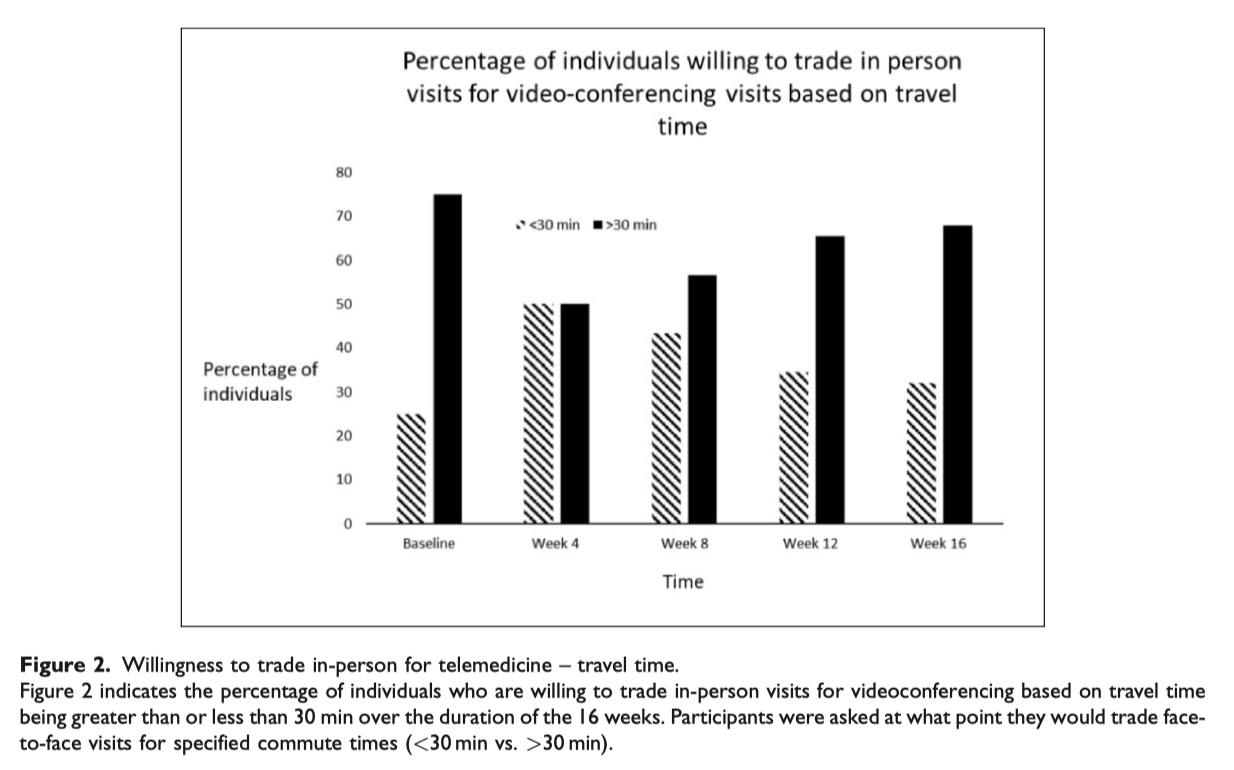
Effective weight-management interventions require frequent interactions with specialised multidisciplinary teams of medical, nutritional and behavioural experts. However, barriers that exist in rural areas, such as transportation and a lack of specialised services, can prevent patients from receiving quality care. We recruited patients from the Dartmouth-Hitchcock Weight & Wellness Center into a single-arm, non-randomised study of a remotely delivered 16-week evidence-based healthy lifestyle programme. Every 4 weeks, participants completed surveys that included their willingness to pay for services like those experienced in the intervention based on commute and copay. Overall, those with a travel duration of 31–45 min had a greater willingness to trade in-person visits for telehealth than any other group. Participants who had a travel duration less than 15 min, 16–30 min and 46–60 min experienced a positive trend in willingness to have telehealth visits until Week 8, where there was a general negative trend in willingness to trade in-person visits for virtual. Participants believed that telemedicine was useful and helpful. In rural areas where patients travel 30–45 min a telemedicine-delivered, intensive weight-loss intervention may be a well-received and cost-effective way for both patients and the clinical care team to connect.

Vanessa K. Rauch, Meredith Roderka, Auden C. McClure, Aaron B. Weintraub, Kevin Curtis, David F. Kotz, Richard I. Rothstein, and John A. Batsis. Willingness to pay for a telemedicine-delivered healthy lifestyle programme. Journal of Telemedicine and Telecare, June 2020. Sage. DOI: 10.1177/1357633X20943337